
How to use this toolkit
The Bipartisan Safer Communities Act (BSCA) is a game changer. It starts with gun safety measures like increased background checks, then it changes the frame entirely as a historic investment into mental health and school-based services. The BSCA expands mental health services in communities and schools, and treats schools as key points for observation and intervention. Furthermore, the BSCA provides schools and states with a path to sustainable, long-term funding through billing for Medicaid school-based services. As pandemic funds expire in the midst of a youth mental health crisis, the BSCA means better support for students, and improved funding and opportunity for educators to support them.
Intro
Medicaid can reimburse states for school-based services if they are covered within the state’s Medicaid State plan or available under the mandatory Early and Periodic Screening Diagnostic and Treatment (EPSDT) requirement The full list of services coverable is in section 1905(a) of the Medicaid statute, 42 USC 1905. Go to reference . As of this publication, roughly half the states have seized the new opportunity to bill for services, meaning half the states have not. But even the states that have taken some action and/or submitted an amended State Plan, still have steps they can take to increase Medicaid billing and the amount of students receiving school-based services.
- 1 The full list of services coverable is in section 1905(a) of the Medicaid statute, 42 USC 1905.
Why School-Based Services Matter
Why School-Based Services Matter
School-based services (SBS) play an essential role in the health of children and adolescents. The school setting offers a unique opportunity to meet children where they are. Children generally spend over 30 hours a week in school during most of the year, and more than 41 million children are currently covered by Medicaid or Children’s Health Insurance Program (CHIP). Schools, early childhood settings and local educational agencies (LEAs) are vital to help support children and their families because they can provide access to important health services right where students spend their days.
Benefits of school-based services include:
- Access to a broad range of health care services. Schools can act as a point of access for preventive services (e.g. immunizations, screenings), behavioral health services (e.g. mental health and substance use disorder (SUD) services), physical and occupational therapy, and disease management for chronic diseases (e.g. obesity, asthma).
- Improved access through reduced travel barriers. Providing services in schools helps reduce the time students miss to attend doctors’ appointments. At the same time, it can decrease disruption of caregivers’ work schedules and concerns with transportation to a health care facility. This is particularly important in light of provider shortages, especially in rural areas.
- Reduced stigma. Increasing the capacity of schools to promote behavioral or mental health services for all students helps create an environment where seeking assistance is more ordinary and customary, and in doing so, drives down the cultural and community stigma and promotes family help-seeking.
- Increase overall health for the entire student body. Schools and early childhood settings can also serve as a catalyst for children, including low-income or under-resourced students, to access primary and preventive services, promoting health and educational equity.
- Positive effects in many aspects of the student’s life. Offering services in school can produce countless positive effects downstream, including increased school attendance, fewer emergency room visits, and reduced health insurance churn for children and their families.
- Assistance in navigating the health care labyrinth. The services that can be offered by schools can help youth obtain personal or family Medicaid and CHIP coverage, access health care services, and connections with community-based organizations and supports.
Historically, one of the biggest obstacles to offering such services is sustainable funding. Now the BSCA offers a way out. With proper implementation, schools can receive reimbursement for costs associated with administering and delivering to children a wide variety of services covered by Medicaid. The details of implementation are described below.
These flexibilities can significantly reduce schools’ administrative burden, making it far easier to receive federal funds for covered health services delivered to children enrolled in Medicaid/CHIP. The changes are especially valuable for small, rural or under-resourced schools.
What the BSCA Does
What the BSCA Does
Medicaid is a partnership between a state and the federal government. States operate the Medicaid program and determine program administration, eligibility, and covered services, within federal statutory and regulatory requirements. Then the federal Centers for Medicare and Medicaid Services (CMS) covers a specified percentage of the state’s total costs. The methods and policies states use to determine how their Medicaid programs operate are described in a written Medicaid State Plan. States can update their plans at their option by submitting a State Plan Amendment (SPA) to CMS for approval.
Prior to 2014, Medicaid only covered SBS for students under an Individualized Education Program (IEP) or an Individualized Family Service Plan (IFSP). After 2014, this rule was clarified and reversed. Medicaid is now allowed to cover SBS for any students—including those with 504 plans or those in general education—who are enrolled in Medicaid for any health services covered according to Early and Periodic Screening, Diagnostic and Treatment (EPSDT) and the State Medicaid plan. The 2014 change was a good start, but schools still needed more flexibility. The BSCA and subsequent agency action, including the 2023 CMS Administrative Claiming Guide offers these needed flexibilities. These flexibilities can significantly reduce schools’ administrative burden, making it far easier to receive federal funds for covered health services delivered to children enrolled in Medicaid/CHIP. The changes are especially valuable for small, rural or under-resourced schools.
What’s more, the BSCA directs agencies to award short-term grants to build infrastructure and create long-term policies and additional flexibility needed to expand access to school-based health and behavioral health services. Benefits include:
Short-term Grants
The U.S. Department of Health and Human Services and the U.S. Department of Education have awarded $1.5 billion in short-term grants, and the U.S. Department of Justice has awarded an additional $60 million. Grant purposes include $500 million for training to increase the pool of skilled professionals providing mental health services in schools, and $285 million for schools to hire and train mental health counselors.
In January 2024, CMS announced a $50 million grant program designed to build capacity among states implementing reforms. CMS expects the award to reach 20 states, split between states that have not yet taken action to cover school-based health services, states that have taken only partial steps in that direction, and states that have expanded. Grants are not a long-term solution, of course, but they can fill gaps and assist schools with infrastructure needs and ability to hire and train mental health professionals, while state Medicaid Plans are amended and new systems are put into place. The current round of grant applications are due by March 25, 2024.
Before the BSCA, according to psychologist.com, “[d]uring the 2019-2020 school year, nearly half of public schools reported not providing diagnostic mental health services for students. And only 42 percent offered mental health treatment services of any kind.” Under the assistance within the BSCA, schools are projected to hire an additional 14,000 mental health professionals over the next 5 years. As of March 2023, compared with the pre-pandemic period, the number of school social workers was up 48%, the number of school nurses increased 42%, and the number of school counselors and school psychologists increased 10%. For tracking ED grants, NEA has provided an online resource.
Sustainable long-term billing for Medicaid SBS
With pandemic funds expiring and grant funds being short-term, Medicaid provides a sustainable long-term funding source for school-based services. States can expand for administrative costs and/or direct costs allowing claiming for administrative and direct services. A wide range of services can be covered, and schools and school districts can customize services to meet their needs. Perhaps they need an audiologist to provide hearing assessments for the entire student body; perhaps they need physical or occupational therapy for individual students. Administrative costs in support of such school-based services might include outreach and enrollment, care coordination, coordination of transportation, coordination of referrals, translation and interpretation services, Medicaid/CHP related training, and more.
Technical Assistance
To assist with training school-based mental health professionals, CMS has created a technical assistance center to provide trainings and educational webinars to help with implementation.
What You Need To Do
What You Need To Do
Access to federal funds does not happen automatically. States must take action! As of this publication, roughly half the states have seized the new opportunity. So roughly half the states have not taken action, and even the states that have taken some action may have still more steps ahead to increase Medicaid billing and the amount of students receiving school-based services.
If it seems like a lot of work and it is too late, know that the CMS $50 million capacity building grant program is open until March 25, 2024.
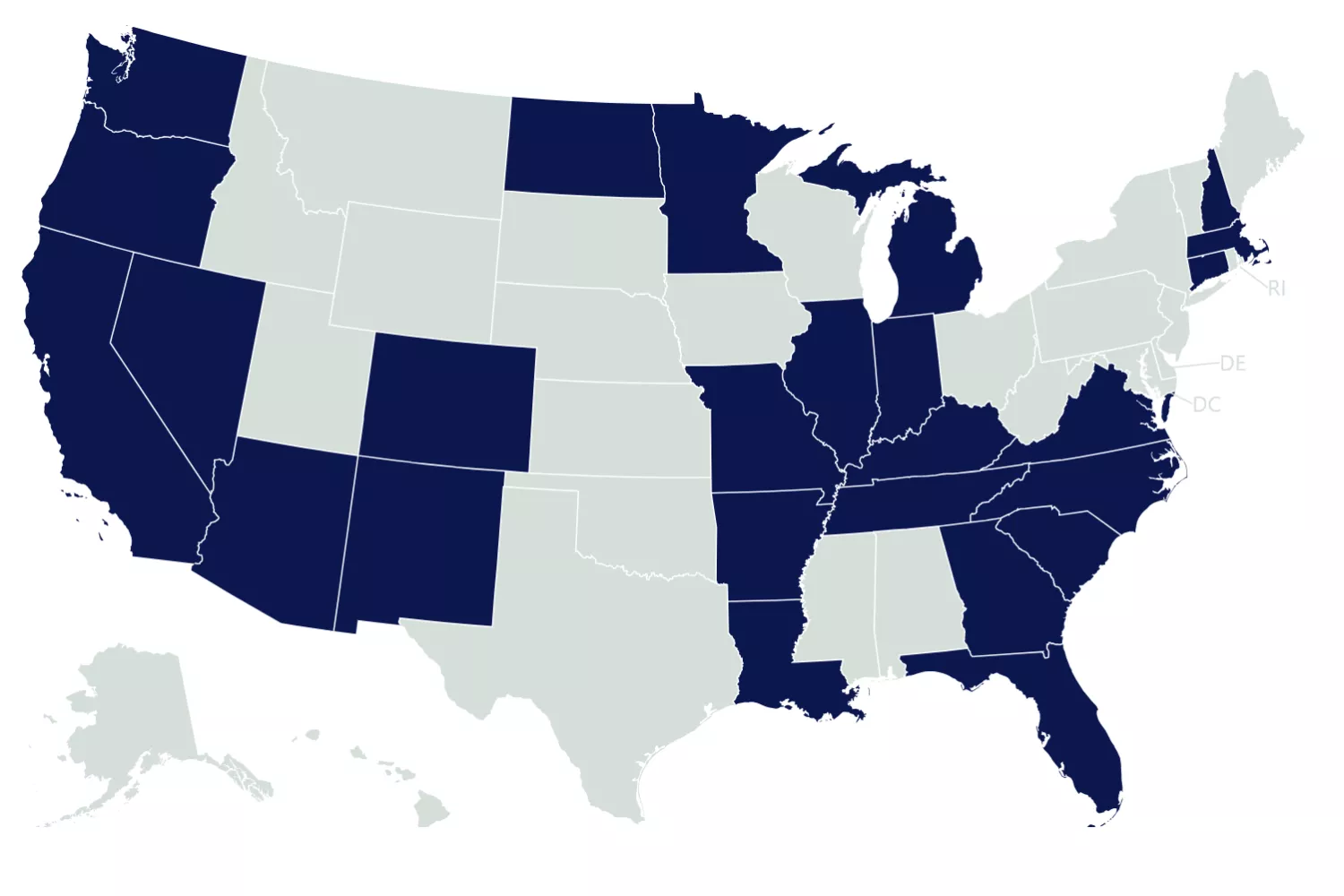
Healthy Students, Promising Futures, Map of School Medicaid Programs
This is what states need to do, based on what they’ve done so far.
1. States that have Taken No Action (CMS refers to these states as “IDEA States” because they only cover students with IEPs or IFSPs)
Next steps for states that have taken no action to expand outside the IEP include:
- Amend State Plan to include School-Based Services and do so in the broadest way possible to include all Medicaid populations, all providers, and all medically necessary and EPSDT services.
- Adopt additional flexibilities under the new CMS Claiming Guide.
- Think through parental consent requirements under the Individuals with Disabilities Education Act (IDEA) and Family Educational Rights and Privacy Act (FERPA) and note potential changes in the CMS proposed rule to the parental consent process for billing.
- Bring more LEAs into the school Medicaid program.
2. States in the Process of Expanding Medicaid Coverage in schools (CMS refers to these States as “partially beyond IDEA”)
Next steps for states that have taken some action, which may include expansion to only some Medicaid populations, or only some services or providers:
- Review the State Plan to determine what amendment is needed to expand to all Medicaid populations, all providers, and all medically necessary and EPSDT services.
- Adopt additional flexibilities under the new CMS Claiming Guide.
- Think through parental consent requirements under the Individuals with Disabilities Education Act (IDEA) and Family Educational Rights and Privacy Act (FERPA) and note potential changes in the CMS proposed rule to the parental consent process for billing.
- Bring more LEAs into the school Medicaid program.
3. States that Expanded Medicaid Coverage in Schools (CMS refers to these States as “fully beyond IDEA”)
States that have already implemented Medicaid school-based support services for all Medicaid-eligible students might still have more to do:
- Adopt additional flexibilities under the new CMS Claiming Guide.
- Think through parental consent requirements under the Individuals with Disabilities Education Act (IDEA) and Family Educational Rights and Privacy Act (FERPA) and note potential changes in the CMS proposed rule to the parental consent process for billing.
- Bring more LEAs into the school Medicaid program.
Additional Resources
Additional Resources
Agency Material
CMS Informational Bulletins
- Leveraging Medicaid, CHIP, and Other Federal Programs in the Delivery of Behavioral Health Services for Children and Youth
- Information on School-Based Services in Medicaid: Funding, Documentation and Expanding Services
- Information on School-Based Services in Medicaid: Policy Flexibilities and Guide on Coverage, Billing, Reimbursement, Documentation and School-Based Administrative Claiming
Claiming Guide
- CMS Informational Bulletin: Information on School-Based Services in Medicaid: Policy Flexibilities and Guide on Coverage, Billing, Reimbursement, Documentation and School-Based Administrative Claiming
- Comprehensive Guide to Medicaid Services and Administrative Claiming (CMS)
- Fact Sheet: Delivering Service in School-based Settings: A Comprehensive Guide to Medicaid Services and Administrative Claiming
Parental Consent
Funding
- Joint Letter with Secretary Xavier Becerra of HHS regarding Federal Resources for Student Mental Health
- CMS Announces $50 Million in Grants to Deliver Critical School-Based Health Services to Children
NEA Material
- NEA released Your Guide to the BSCA that details how affiliates can work with State decision makers to use the BSCA to increase mental health and other services for students.
- NEA Collective Bargaining and Member Advocacy (CBMA) created resources entitled Bargaining and Advocating to Support Our Members’ Mental Health and Bargaining for Gun Safety.
- NEA Resource to locate ED Grants
General Background
- Healthy Schools Campaign Guide to Expanding Medicaid Funding School Health Services
- Healthy Schools Campaign Tracking Map
- Healthy Schools Campaign – State Medicaid Education Standards for School Health Personnel
- Healthy Schools Campaign Webinar Series
- Healthy Students Promising Futures – Financial Impact of Expanding School Medicaid Programs
Technical Assistance
- CMS and ED have offered to review SPAs prior to submitting and offer assistance on SBS guidance. States should contact CMS to discuss these flexibilities PRIOR to submitting any SPAs, administrative claiming plan amendments, and/or amendments to time study implementation plans at [email protected]
- Technical Assistance Center is operational and expanding, and available to SEAs and LEAs
Downloads
Learn More





Use Your Educator Voice.
